
Fact Checked
This article has been fact checked by a licensed expert before publication to ensure all information provided is correct and safe.
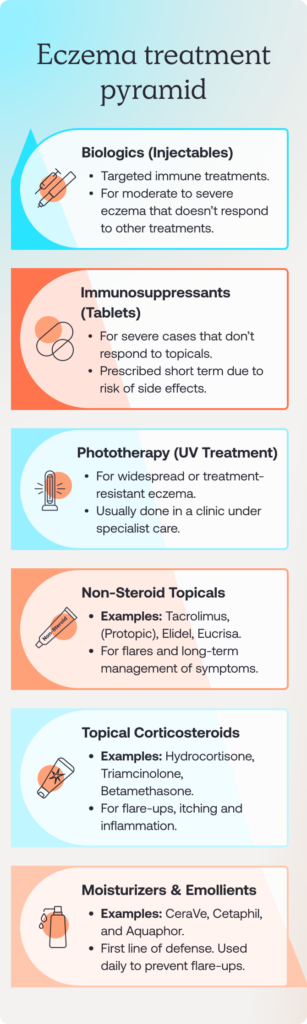
How are different types of eczema treated?

Medically reviewed by
Alexandra Cristina Cowell, Writer & Clinical Content Reviewer
Medically reviewed by
Dr Alexandra Cristina Cowell
Writer & Clinical Content Reviewer
on May 29, 2025.
Meet Alexandra Cristina
Last updated on Feb 20, 2026.













Find treatment



Popular treatments







I'm looking for
Popular searches:
Sign up to our newsletter for all the latest on Atopic eczema and more.
By clicking 'Subscribe now' you're agreeing to our Privacy Policy.